THE SAFETY OF KISUNLA IN CLINICAL TRIALS*
Adverse Reactions Reported In TRAILBLAZER-ALZ 6 At 52 Weeks1,2†‡

TRAILBLAZER-ALZ 6 reported adverse reactions in the original Kisunla dosing group (n=207) vs the Kisunla gradual-titration group (n=212; gradual-titration dosing was 350 mg for the first dose, 700 mg for the second dose, and 1050 mg for the third dose, followed by 1400 mg every 4 weeks [Q4W]). TRAILBLAZER-ALZ 6 adverse reactions reported included:
Amyloid-related imaging abnormalities (ARIA) (including asymptomatic radiographic events): 34% with Kisunla original dosing vs 29% with Kisunla gradual-titration dosing.
Amyloid-related imaging abnormalities-edema (ARIA-E): 25% with Kisunla original dosing vs 16% with Kisunla gradual-titration dosing.
Amyloid-related imaging abnormalities-hemosiderin deposition (ARIA-H): 28% with Kisunla original dosing vs 25% with Kisunla gradual-titration dosing.
ARIA-H microhemorrhage: 21% with Kisunla original dosing vs 23% with Kisunla gradual-titration dosing.
ARIA-H superficial siderosis: 15% with Kisunla original dosing vs 8% with Kisunla gradual-titration dosing.
Headache: 21% with Kisunla original dosing vs 18% with Kisunla gradual-titration dosing.
Infusion-related reaction (IRR): 14% with Kisunla original dosing vs 16% with Kisunla gradual-titration dosing.
aIn TRAILBLAZER-ALZ 6, placebo was given every other visit to preserve blinding for additional arms (not shown) to explore pharmacokinetics.3
bGradual-titration dosing was 350 mg for the first dose, 700 mg for the second dose, and 1050 mg for the third dose, followed by 1400 mg Q4W.1
†In TRAILBLAZER-ALZ 6, ARIA (including asymptomatic radiographic events) was observed in 34% of participants treated with the original dosing regimen compared with 29% of participants treated with gradual-titration dosing.2
‡Clinical symptoms associated with ARIA-E resolved in approximately 90% of patients in the original dosing arm compared to 67% of patients in the gradual-titration arm.4
The primary endpoint of TRAILBLAZER-ALZ 6 was the proportion of participants with any occurrence of ARIA-E1
-
Significant reduction of ARIA-E with gradual-titration dosing1
- 16% of patients in the gradual-titration arm vs 25% of patients in the original dosing arm1
- Approximately 84% of participants in the gradual-titration arm had no ARIA-E on MRI through week 525
- Symptomatic ARIA-E was observed in 5% of patients in the original dosing arm compared to 3% of patients in the gradual-titration arm4
- Less than 1% of patients treated with Kisunla experienced any ARIA that led to serious outcomes, such as hospitalization or medical intervention4
*The safety of Kisunla has been evaluated in 3727 patients with Alzheimer's disease (AD) who received at least 1 dose of Kisunla intravenously across 2 Phase 3 clinical trials.1
Adverse reactions reported in TRAILBLAZER-ALZ 2 at 76 weeks1
Adverse reactions reported in ≥5% of patients treated with Kisunla (n=853) and ≥2% higher than placebo (n=874) in TRAILBLAZER-ALZ 2 at 76 weeks. The incidence of ARIA-H in TRAILBLAZER-ALZ 2 was 31% in patients treated with Kisunla vs 13% in patients treated with placebo. ARIA-H microhemorrhage (25% vs 11%), amyloid-related imaging abnormalities-edema (ARIA-E) (24% vs 2%), ARIA-H superficial siderosis (15% vs 3%), headache (13% vs 10%), and infusion-related reactions (IRR) (9% vs 0.5%). ARIA (including asymptomatic radiographic events) was observed in 36% of participants treated with Kisunla compared to 14% of participants treated with placebo.1
- Less than 2% of patients treated with Kisunla experienced ARIA that led to serious outcomes6
- Symptomatic ARIA-E was observed in 6% of patients treated with Kisunla compared to 0% of patients treated with placebo1
- Clinical symptoms associated with ARIA-E resolved in approximately 85% of patients taking Kisunla1
Original dosing was 700 mg for the first, second, and third dose (700/700/700 mg), followed by 1400 mg every 4 weeks (Q4W). This is the previously approved dosing regimen.1 Please refer to package insert for dosing instructions.
ARIA-E includes brain edema or sulcal effusions. ARIA-H most commonly includes macrohemorrhage and superficial siderosis.1
For your patients with early symptomatic Alzheimer’s disease (AD) and confirmed amyloid positivity1:
GRADUAL-TITRATION DOSING1
In TRAILBLAZER-ALZ 6, alternative dosing regimens with Kisunla were assessed. The primary endpoint was the proportion of participants with any occurrence of ARIA-E.1
Assessed the impact of gradual-titration dosing* on ARIA-E frequency and amyloid plaque reduction1
- Participants (N=842) were randomized to 1 of 4 alternative Kisunla dosing regimens in a 1:1:1:1 ratio†, including:
- Original dosing (N=207)‡: Consistent with TRAILBLAZER-ALZ 2
- Gradual-titration dosing (N=212): 350 mg for the first dose, 700 mg for the second dose, 1050 mg for the third dose, followed by 1400 mg every 4 weeks (Q4W)
Inclusion and exclusion criteria were the same as TRAILBLAZER-ALZ 2 except that tau PET was not an inclusion criterion.1
*The treatment period was up to 72 weeks; treatment stopping criteria based on amyloid PET were the same as TRAILBLAZER-ALZ 2.1
†1:1:1:1 randomization stratified by ApoE ε4 carrier status and by baseline amyloid PET. For the original and gradual-titration dosing arms, placebo was given every other week for the first 16 weeks to preserve blinding for additional arms (not shown) to explore pharmacokinetics.3
‡Original dosing was 700 mg for the first, second, and third dose (700/700/700 mg), followed by 1400 mg Q4W.1
ApoE ε4=apolipoprotein E type 4 allele; ARIA=amyloid-related imaging abnormalities; ARIA-E=amyloid-related imaging abnormalities-edema; PET=positron emission tomography.
SELECT IMPORTANT SAFETY INFORMATION
Risk Factors for ARIA and Intracerebral Hemorrhages (ICH)
- Radiographic Findings of Cerebral Amyloid Angiopathy (CAA): Neuroimaging findings that may indicate CAA include evidence of prior ICH, cerebral microhemorrhage, and cortical superficial siderosis. CAA has an increased risk for ICH. The presence of an ApoE ε4 allele is also associated with CAA.
- The baseline presence of at least 2 microhemorrhages or the presence of at least 1 area of superficial siderosis on MRI, which may be suggestive of CAA, were identified as risk factors for ARIA. Patients were excluded from enrollment for findings on neuroimaging of prior ICH >1 cm in diameter, >4 microhemorrhages, >1 area of superficial siderosis, severe white matter disease, and vasogenic edema.
ARIA=amyloid-related imaging abnormalities; ARIA-E=amyloid-related imaging abnormalities-edema; ARIA-H=amyloidrelated imaging abnormalities-hemosiderin deposition; MRI=magnetic resonance imaging.
In TRAILBLAZER-ALZ 6, gradual-titration dosing reduced the frequency of ARIA-E compared to the original dosing1
REDUCED ARIA-E RADIOGRAPHIC SEVERITY WAS SEEN IN THE GRADUAL-TITRATION* ARM COMPARED TO THE ORIGINAL DOSING† ARM IN TRAILBLAZER-ALZ 61
ARIA-E Severity Distribution Shifted Toward None or Less Severe in the Gradual-Titration Arm1,5
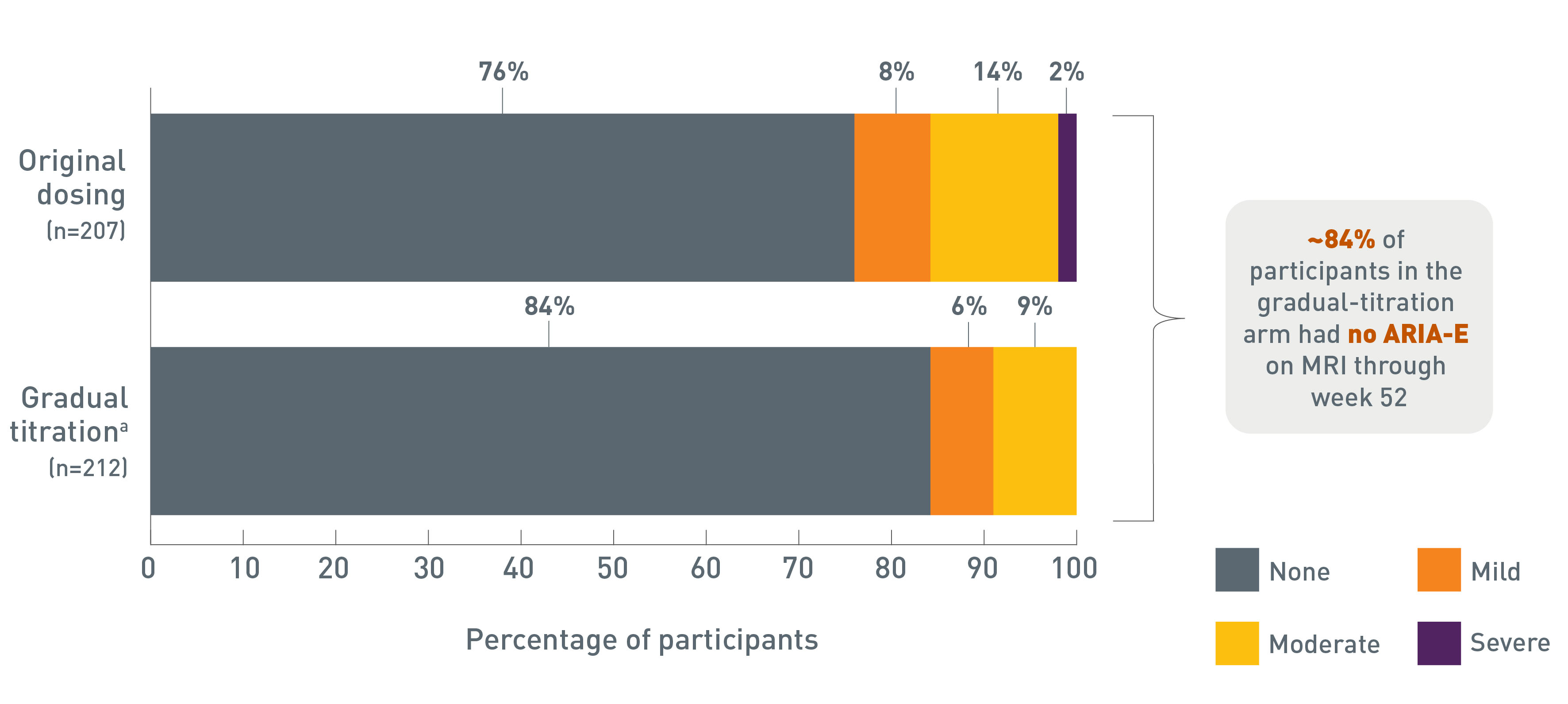
Bar graph showing the distribution of amyloid-related imaging abnormalities-edema (ARIA-E) maximum radiographic severity shifted toward none or less severe in the TRAILBLAZER-ALZ 6 gradual-titration arm (n=212) compared with the original-dosing arm (n=207). In the gradual-titration arm, the maximum radiographic severity of ARIA-E in participants treated with Kisunla was mild in 6% (13/212) of participants, moderate in 9% (20/212) of participants, and severe in 0% (0/212) of participants. 84% (179/212) of participants had no ARIA-E through week 52. In the original dosing arm, the maximum radiographic severity of ARIA-E in participants treated with Kisunla was mild in 8% (17/207) of participants, moderate in 14% (29/207) of participants, and severe in 2% (4/207) of participants. 76% (157/207) of participants had no ARIA-E through week 52.
aDue to rounding, numbers presented may not add up to the totals indicated, and percentages may not reflect the absolute figures for the same reason.
In patients taking Kisunla in TRAILBLAZER-ALZ 6 at 52 weeks5:
- Maximum radiographic severity of ARIA-H microhemorrhage and ARIA-H superficial siderosis in patients in the gradual-titration arm were, respectively: mild: 18% (37/212) and 4% (9/212); moderate: 3% (6/212) and 3% (6/212); and severe: 2% (5/212) and 1% (3/212)
- Maximum radiographic severity of ARIA-H microhemorrhage and ARIA-H superficial siderosis in patients in the original dosing arm were, respectively: mild: 14% (28/207) and 9% (18/207); moderate: 5% (10/207) and 2% (4/207); and severe: 3% (6/207) and 4% (9/207)
In TRAILBLAZER-ALZ 2 at 76 weeks5:
- Maximum radiographic severity of ARIA-E in patients taking Kisunla; mild: 7% (59/853); moderate: 15% (128/853); and severe: 2% (14/853). Maximum radiographic severity of ARIA-E in patients on placebo: mild: 2% (14/874); moderate: 0.3% (3/874); and severe: 0% (0/874)
- Maximum radiographic severity of ARIA-H microhemorrhage and ARIA-H superficial siderosis for patients taking Kisunla, respectively: mild: 17% (143/853) and 6% (47/853); moderate: 4% (34/853) and 4% (32/853); and severe: 5% (40/853) and 5% (46/853). Maximum radiographic severity of ARIA-H microhemorrhage and ARIA-H superficial siderosis for patients on placebo, respectively: mild: 10% (88/874) and 2% (16/874); moderate: 1% (11/874) and 1% (5/874); and severe: 0.1% (1/874) and 0.2% (2/874)
*Gradual-titration dosing was 350 mg for the first dose, 700 mg for the second dose, and 1050 mg for the third dose, followed by 1400 mg Q4W.1
†Original dosing was 700 mg for the first, second, and third dose (700/700/700 mg), followed by 1400 mg Q4W. This is the previously approved dosing regimen.1 Please refer to the package insert for dosing instructions.
ARIA=amyloid-related imaging abnormalities; ARIA-E=amyloid-related imaging abnormalities-edema; ARIA-H=amyloid-related imaging abnormalities-hemosiderin deposition; MRI=magnetic resonance imaging.
SELECT IMPORTANT SAFETY INFORMATION
WARNING: AMYLOID-RELATED IMAGING ABNORMALITIES
Monoclonal antibodies directed against aggregated forms of beta amyloid, including Kisunla, can cause amyloid-related imaging abnormalities (ARIA), characterized as ARIA with edema (ARIA-E) and ARIA with hemosiderin deposition (ARIA-H). ARIA usually occurs early in treatment and is usually asymptomatic, although serious and life-threatening events can occur. ARIA can be fatal. Serious intracerebral hemorrhages >1 cm, some of which have been fatal, have been observed in patients treated with this class of medications. Because ARIA-E can cause focal neurologic deficits that can mimic an ischemic stroke, treating clinicians should consider whether such symptoms could be due to ARIA-E before giving thrombolytic therapy in a patient being treated with Kisunla.
ApoE ε4 Homozygotes: Patients who are apolipoprotein E ε4 (ApoE ε4) homozygotes treated with this class of medications, including Kisunla, have a higher incidence of ARIA, including symptomatic, serious, and severe radiographic ARIA, compared to heterozygotes and noncarriers. Testing for ApoE ε4 status should be performed prior to initiation of treatment to inform the risk of developing ARIA. Prior to testing, the risk of ARIA across genotypes and implications of genetic testing results should be discussed with patients.
Consider the benefit for the treatment of Alzheimer's disease and risk of ARIA when deciding to treat with Kisunla.
RATES OF ARIA-E ACROSS ApoE ε4 GENOTYPES
TRAILBLAZER-ALZ 6 at 52 Weeks1
Percentage of participants with ARIA-E through 52 weeks
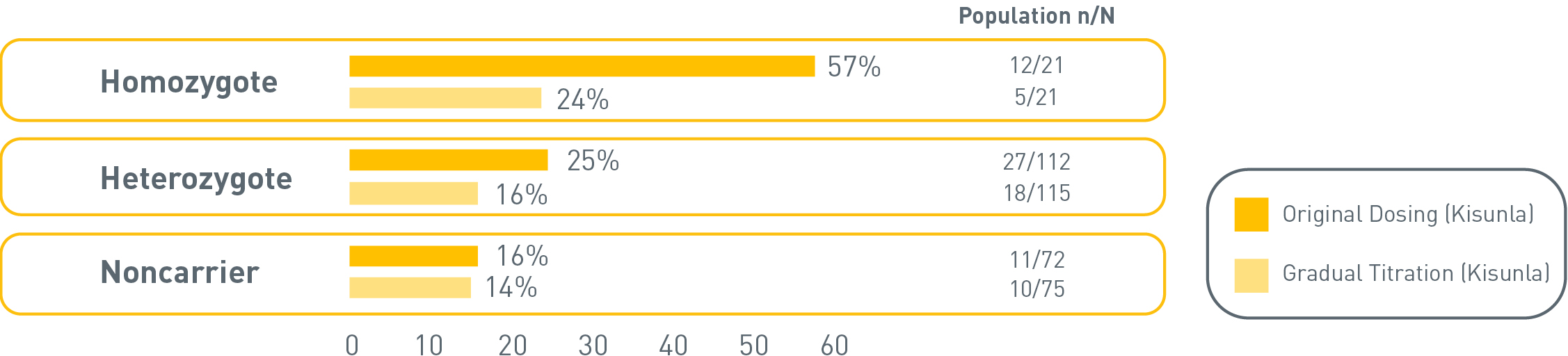
The incidence of ARIA-E was 24% (5/21) in ApoE ε4 homozygotes for gradual-titration dosing vs 57% (12/21) for original dosing, 16% (18/115) in heterozygotes for gradual-titration dosing vs 25% (27/112) for original dosing, and 14% (10/75) in noncarriers for gradual-titration dosing vs 16% (11/72) for original dosing.
The small number of events and limited exposure in the ApoE ε4 subgroups limit definitive conclusions about the risk of ARIA-E.
In TRAILBLAZER-ALZ 6, ApoE ε4 homozygotes saw reduced rates of ARIA-E from 57% (original dosing) to 24% (gradual-titration dosing).1
In TRAILBLAZER-ALZ 2, of patients in the Kisunla arm (n=850), 17% (n=143) were ApoE ε4 homozygotes, 53% were heterozygotes (n=452), and 30% (n=255) were noncarriers. The incidence of ARIA through 76 weeks was higher in ApoE ε4 homozygotes (55% on Kisunla vs 22% on placebo) than in heterozygotes (36% on Kisunla vs 13% on placebo) and noncarriers (25% on Kisunla vs 12% on placebo).1
Learn about ApoE ε4 genetic testing and the risk of ARIA
ApoE ε4=apolipoprotein E type 4 allele; ARIA=amyloid- related imaging abnormalities; ARIA-E=amyloid-related imaging abnormalities-edema.
ARIA MANAGEMENT
Dosing Recommendations for Patients With ARIA-E1
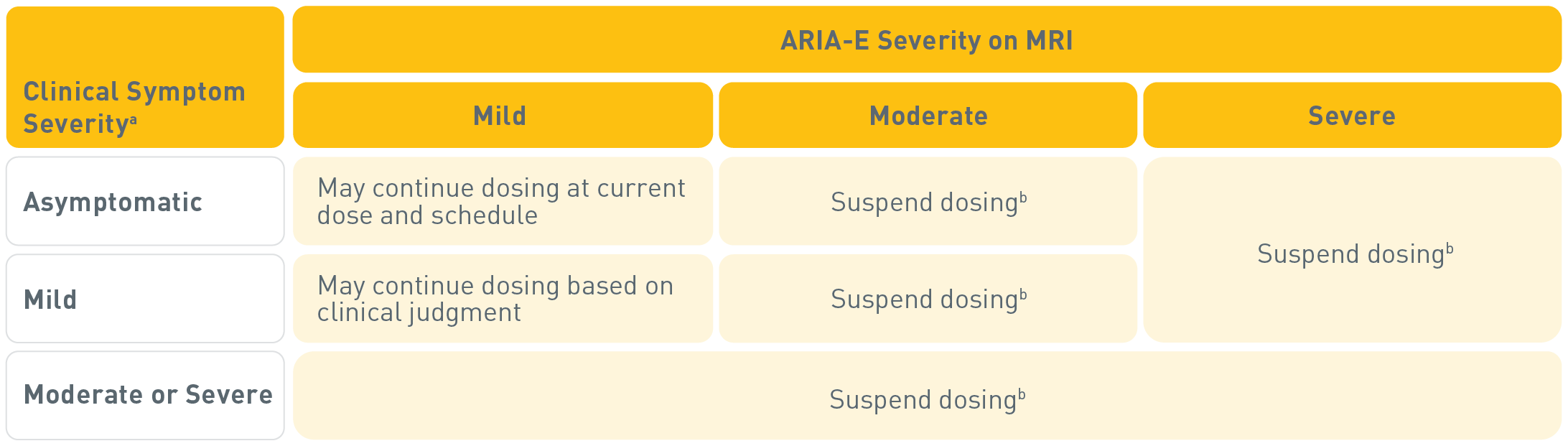
For asymptomatic or mild clinical symptomsa with ARIA-E and mild severity on MRI, dosing may continue based on clinical judgment. For moderate or severe clinical symptoms with ARIA-E, or for moderate or severe ARIA-E on MRI, suspend dosing.b
aMild: discomfort noticed, but no disruption of normal daily activity; Moderate: discomfort sufficient to reduce or affect normal daily activity; Severe: incapacitating, with inability to work or to perform normal daily activity.1
bSuspend until MRI demonstrates radiographic resolution and symptoms, if present, resolve; consider a follow-up MRI to assess for resolution 2 to 4 months after initial identification. Resumption of dosing should be guided by clinical judgment.1
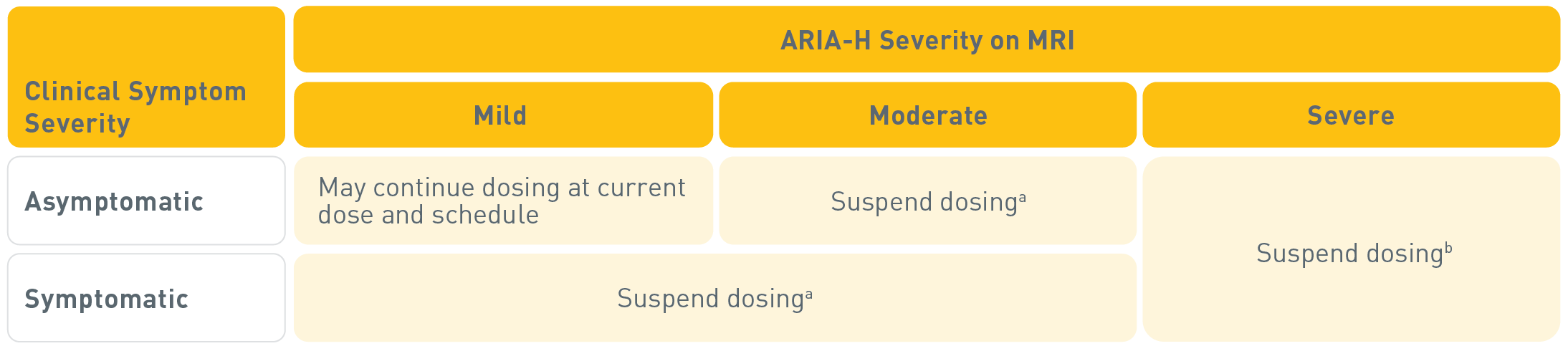
For asymptomatic ARIA-H with mild severity on MRI, dosing may continue at current dose and schedule. For symptomatic ARIA-H, or for moderate or severe ARIA-H on MRI, suspend dosing.1,a,b
aSuspend until MRI demonstrates radiographic stabilization and symptoms, if present, resolve; resumption of dosing should be guided by clinical judgment; consider a follow-up MRI to assess for stabilization 2 to 4 months after initial identification.1
bSuspend until MRI demonstrates radiographic stabilization and symptoms, if present, resolve. Use clinical judgment when considering whether to continue treatment or permanently discontinue Kisunla.1
In patients who develop intracerebral hemorrhage >1 cm in diameter during treatment with Kisunla, suspend dosing until MRI demonstrates radiographic stabilization and symptoms, if present, resolve. Use clinical judgment when considering whether to continue treatment or permanently discontinue Kisunla after radiographic stabilization and resolution of symptoms.1
ARIA=amyloid-related imaging abnormalities; ARIA-E=amyloid-related imaging abnormalities-edema; ARIA-H=amyloid related imaging abnormalities-hemosiderin deposition; MRI=magnetic resonance imaging.
References:
- Kisunla (donanemab-azbt). Prescribing Information. Lilly USA, LLC.
- Data on File. Lilly USA, LLC. DOF-DN-US-0084.
- Wang H, Serap Monkul Nery E, Ardayfio P, et al. Alzheimers Dement. 2025;21(4):e70062. doi:10.1002/alz.70062
- Data on File. Lilly USA, LLC. DOF-DN-US-0085.
- Data on File. Lilly USA, LLC. DOF-DN-US-0081.
- Sims JR, Zimmer JA, Evans CD, et al; for TRAILBLAZER-ALZ 2 Investigators. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527.