
A PHASE 3 STUDY THAT ASSESSED DISEASE PROGRESSION IN EARLY SYMPTOMATIC ALZHEIMER’S DISEASE (AD) BY REDUCING AMYLOID PLAQUES1,2
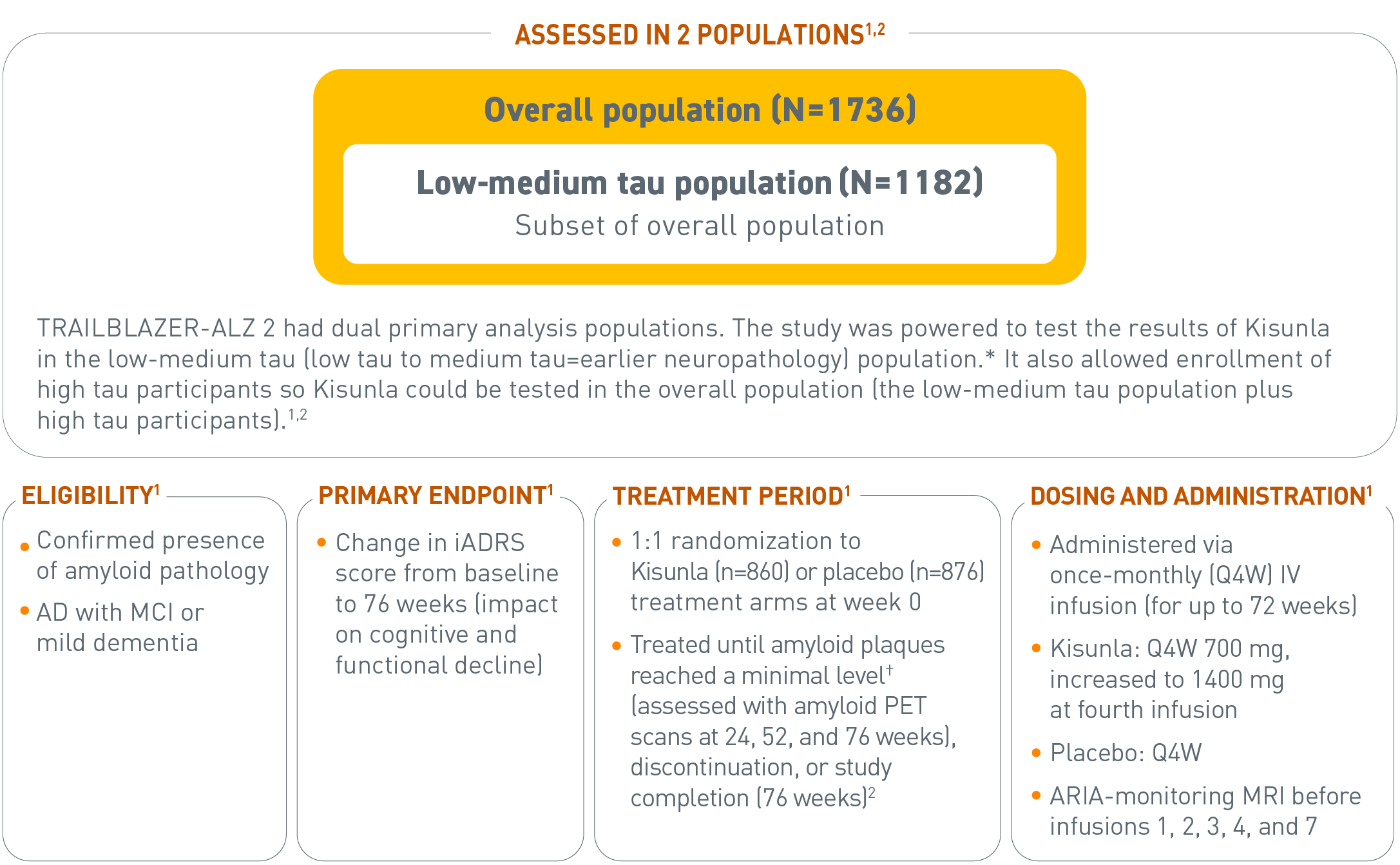
Overall population (N=1736). Low-medium tau population (N=1182). Subset of overall population.
*There were 2 primary analysis populations based on tau PET imaging with flortaucipir: 1) low-medium tau level population (SUVR of ≥1.10 and ≤1.46), and 2) combined population of low-medium plus high tau (SUVR >1.46).1
†In the protocol, if the amyloid plaque level was <11 Centiloids on a single PET scan or 11 to <25 Centiloids on 2 consecutive PET scans, the patient was eligible to be switched to placebo.1
‡The full Prescribing Information recommends ARIA-monitoring MRI before infusions 1, 2, 3, 4, and 7.1
For reference, <24.1 Centiloids on an amyloid PET scan is consistent with a negative visual read.3
ARIA=amyloid-related imaging abnormalities; iADRS=integrated Alzheimer’s Disease Rating Scale; IV=intravenous; MCI=mild cognitive impairment; MRI=magnetic resonance imaging; PET=positron emission tomography; Q4W=every 4 weeks; SUVR=standardized uptake value ratio.
SELECT IMPORTANT SAFETY INFORMATION
Risk Factors for ARIA and Intracerebral Hemorrhages (ICH)
- Radiographic Findings of Cerebral Amyloid Angiopathy (CAA): Neuroimaging findings that may indicate CAA include evidence of prior ICH, cerebral microhemorrhage, and cortical superficial siderosis. CAA has an increased risk for ICH. The presence of an ApoE ε4 allele is also associated with CAA.
- The baseline presence of at least 2 microhemorrhages or the presence of at least 1 area of superficial siderosis on MRI, which may be suggestive of CAA, were identified as risk factors for ARIA. Patients were excluded from enrollment for findings on neuroimaging of prior ICH >1 cm in diameter, >4 microhemorrhages, >1 area of superficial siderosis, severe white matter disease, and vasogenic edema.
KISUNLA GIVES YOU THE POWER TO HELP SLOW COGNITIVE AND FUNCTIONAL DECLINE IN PATIENTS WITH EARLY SYMPTOMATIC AD1,2,4
Low-Medium Tau Population: iADRS Change From Baseline Through 76 Week1,2,4,a,b
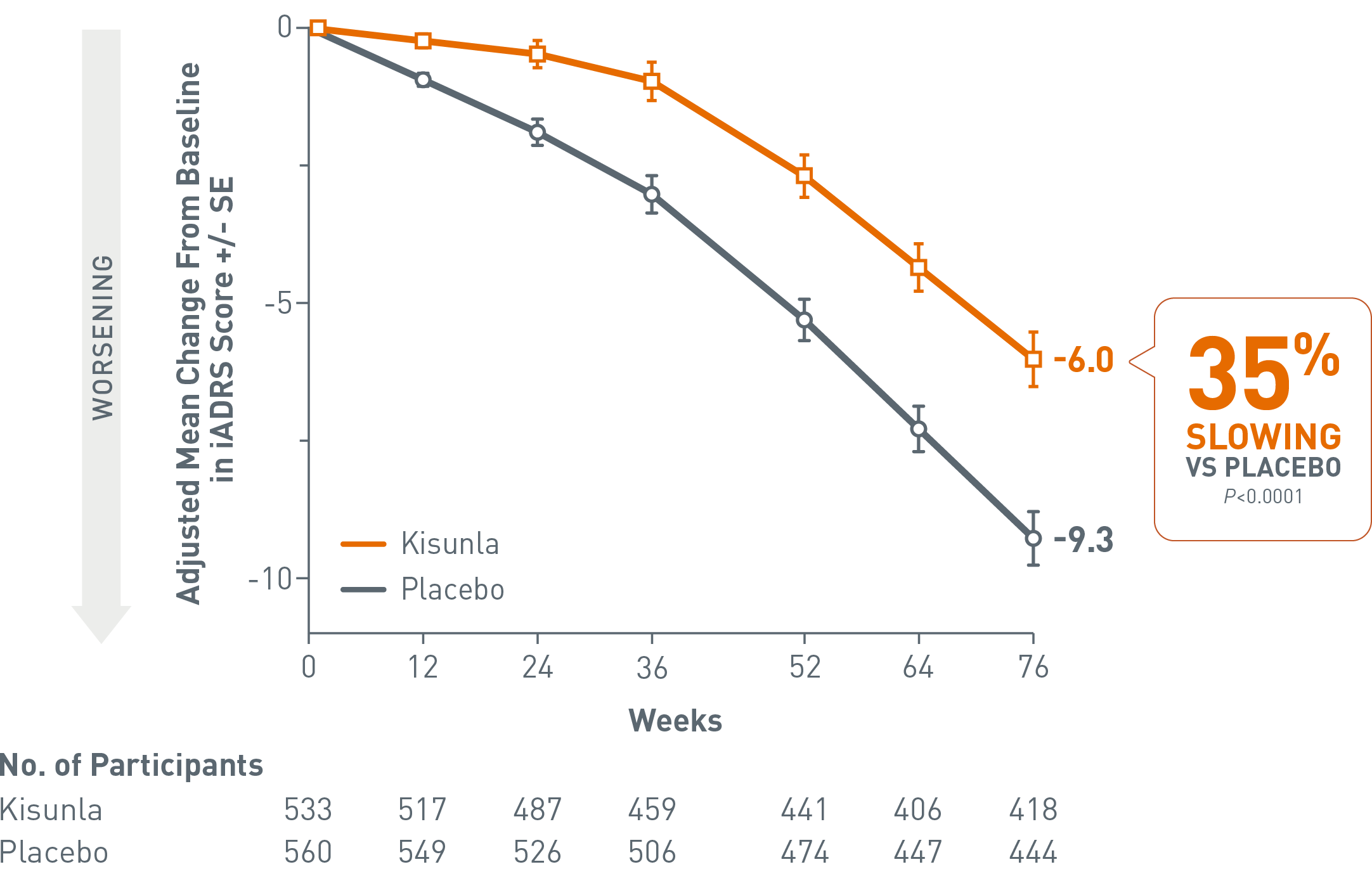
aAssessed using NCS2 analysis.2
bMean baseline Kisunla: 105.92; mean baseline placebo: 105.95.2
Participants treated with Kisunla in the low-medium tau population had statistically significantly less decline in cognition/function than patients treated with placebo as assessed by the iADRS at week 76 (Kisunla: n=418; placebo: n=444). At week 76, adjusted mean change from baseline for patients treated with Kisunla was -6.0 vs -9.3 for placebo. The adjusted mean change difference from placebo was 3.3 (35%); P<0.0001.1,2,4
Overall Population: iADRS Change From Baseline Through 76 Weeks1,2,4,a,b
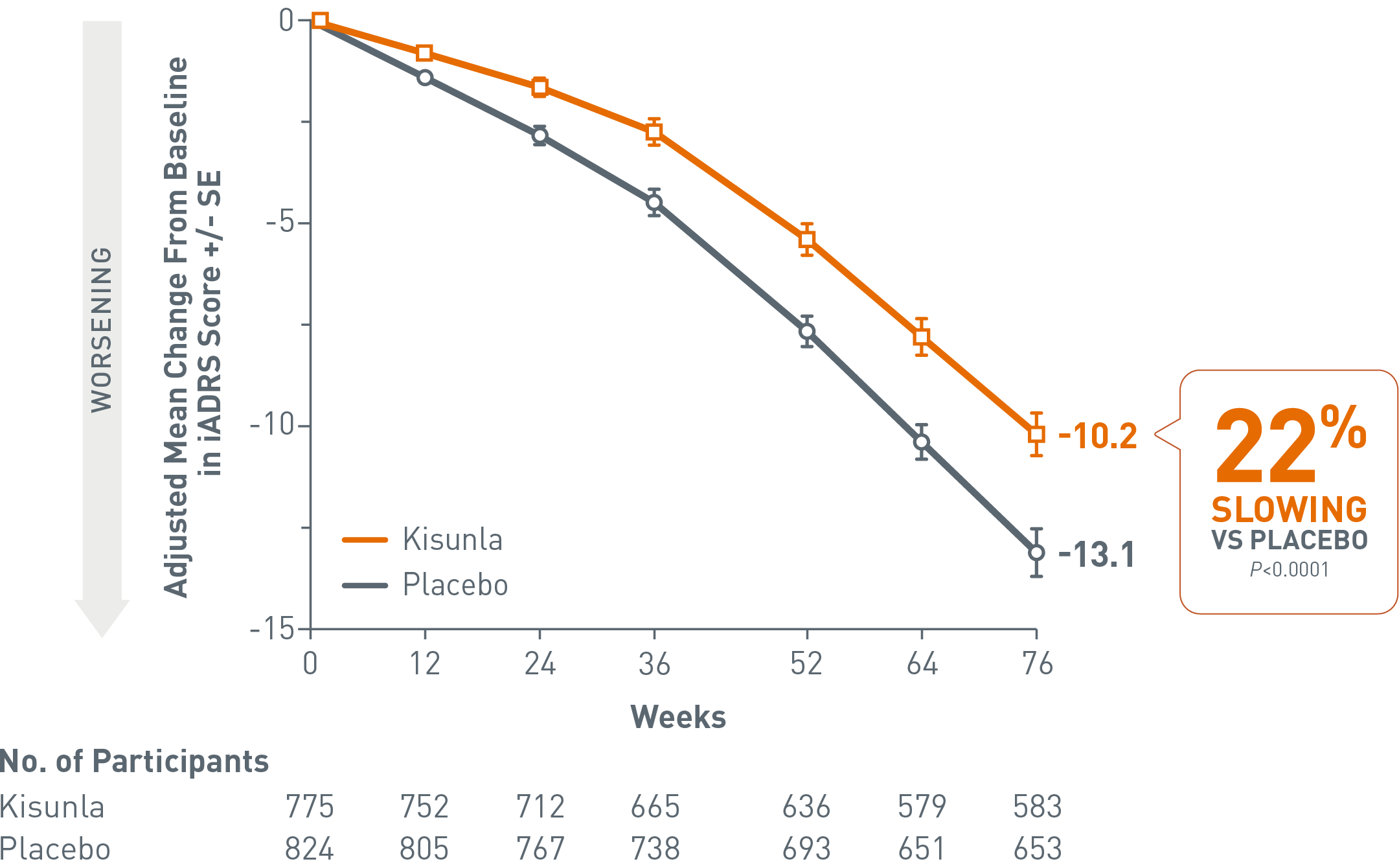
aAssessed using NCS2 analysis.2
bMean baseline Kisunla: 104.55; mean baseline placebo: 103.82.2
Participants treated with Kisunla in the overall population had statistically significantly less decline in cognition/function than patients treated with placebo as assessed by the iADRS at week 76 (Kisunla: n=583; placebo: n=653). At week 76, adjusted mean change from baseline for patients treated with Kisunla was -10.2 vs -13.1 for placebo. The adjusted mean change difference from placebo was 2.9 (22%); P<0.0001.1,2,4
iADRS scores range from 0 to 144 with lower scores indicating greater impairment.1
iADRS=integrated Alzheimer’s Disease Rating Scale; NCS2=natural cubic spline with 2 degrees of freedom; SE=standard error.
HELP KEEP YOUR PATIENTS IN THE EARLIER STAGES OF DISEASE LONGER2
Overall Population (N=1736): Reduction in Risk of Progression* on CDR-GS1
In the overall population (N=1736), 37% reduced risk of progressing to the next stage of disease vs placebo through 76 weeks; P<0.001.2
CDR-GS: Time to worsening of disease
- HR: Overall population=0.63†; 95% CI: 0.51, 0.77; low-medium tau=0.61†; 95% CI: 0.47, 0.802
- In the low-medium tau population, a 39% reduced risk vs placebo was observed through 76 weeks (N=1182); P<0.0012
*Progression to next clinical stage was defined as any increase in CDR-GS at 2 consecutive visits from baseline. 0=normal; 0.5=very mild dementia; 1=mild dementia; 2=moderate dementia; 3=severe dementia.2
†The HR is the relative risk reduction for substantial decline achieved by Kisunla vs placebo.2
CDR-GS=Clinical Dementia Rating Scale-Global Score; CI=confidence interval; HR=hazard ratio.
RISK OF PROGRESSION* TO MODERATE OR SEVERE ALZHEIMER’S DISEASE (AD) OVER 76 WEEKS IN THE OVERALL POPULATION5,6
Reduced Risk of Progression2,5,6
Limitations: This post hoc exploratory analysis was not adjusted for multiplicity; as such, no conclusions can be drawn.

50% lower risk of progressing to moderate or severe AD vs placebo through 76 weeks; HR=0.504 (the HR is the proportional risk for substantial decline achieved by Kisunla vs placebo).
aThe HR is the proportional risk for substantial decline achieved by Kisunla vs placebo.2,5
A post hoc analysis showed that participants treated with Kisunla in the overall population (n=784) had a 50% reduced risk of progressing to moderate or severe AD compared with participants treated with placebo (n=821).2,5,6
*Progression to moderate or severe AD was defined as CDR-GS score of 2 or above at 2 consecutive visits.5,6
CDR-GS=Clinical Dementia Rating-Global Score; HR=hazard ratio.
SELECT IMPORTANT SAFETY INFORMATION
WARNING: AMYLOID-RELATED IMAGING ABNORMALITIES
Monoclonal antibodies directed against aggregated forms of beta amyloid, including Kisunla, can cause amyloid-related imaging abnormalities (ARIA), characterized as ARIA with edema (ARIA-E) and ARIA with hemosiderin deposition (ARIA-H). ARIA usually occurs early in treatment and is usually asymptomatic, although serious and life-threatening events can occur. ARIA can be fatal. Serious intracerebral hemorrhages >1 cm, some of which have been fatal, have been observed in patients treated with this class of medications. Because ARIA-E can cause focal neurologic deficits that can mimic an ischemic stroke, treating clinicians should consider whether such symptoms could be due to ARIA-E before giving thrombolytic therapy in a patient being treated with Kisunla.
ApoE ε4 Homozygotes: Patients who are apolipoprotein E ε4 (ApoE ε4) homozygotes treated with this class of medications, including Kisunla, have a higher incidence of ARIA, including symptomatic, serious, and severe radiographic ARIA, compared to heterozygotes and noncarriers. Testing for ApoE ε4 status should be performed prior to initiation of treatment to inform the risk of developing ARIA. Prior to testing, the risk of ARIA across genotypes and implications of genetic testing results should be discussed with patients.
Consider the benefit for the treatment of Alzheimer's disease and risk of ARIA when deciding to treat with Kisunla.
A LONG-TERM EXTENSION STUDY ASSESSED EFFICACY AND SAFETY FOR UP TO 3 YEARS7
PHASE 3 LONG-TERM EXTENSION (LTE) PERIOD
TRAILBLAZER-ALZ 2 LTE is a Phase 3, double-blind, 78-week extension study evaluating the efficacy and safety of Kisunla for up to 154 weeks. Participants who completed TRAILBLAZER-ALZ 2 (Kisunla or placebo arm) and were eligible as determined at study initiation could continue in the LTE period. Participants on Kisunla in TRAILBLAZER-ALZ 2 continued into the LTE period receiving either Kisunla or placebo based on amyloid reduction to minimal levels* (n=550). Participants on placebo in TRAILBLAZER-ALZ 2 switched to Kisunla in the LTE period (n=657). Of those who received active treatment in the LTE period, participants received Kisunla with the same dosing, administration and stopping criteria as in TRAILBLAZER-ALZ 2.7
PET=positron emission tomography.
*In the study, if the amyloid plaque level was < 11 Centiloids on a single PET scan or 11 to <25 Centiloids on 2 consecutive PET scans, the patient was eligible to be switched to placebo.1
For reference, <24.1 Centiloids on an amyloid PET scan is consistent with a negative visual read.3
PATIENTS TREATED ON KISUNLA SHOWED INCREASING CDR‑SB SEPARATION OVER 3 YEARS8
85% of participants who started Kisunla in the Core Study and continued into the LTE met trial completion criteria based on amyloid PET within 3 years9
CDR-SB Change From Baseline In Cognition And Function Through 3 Years: Overall Population1,8
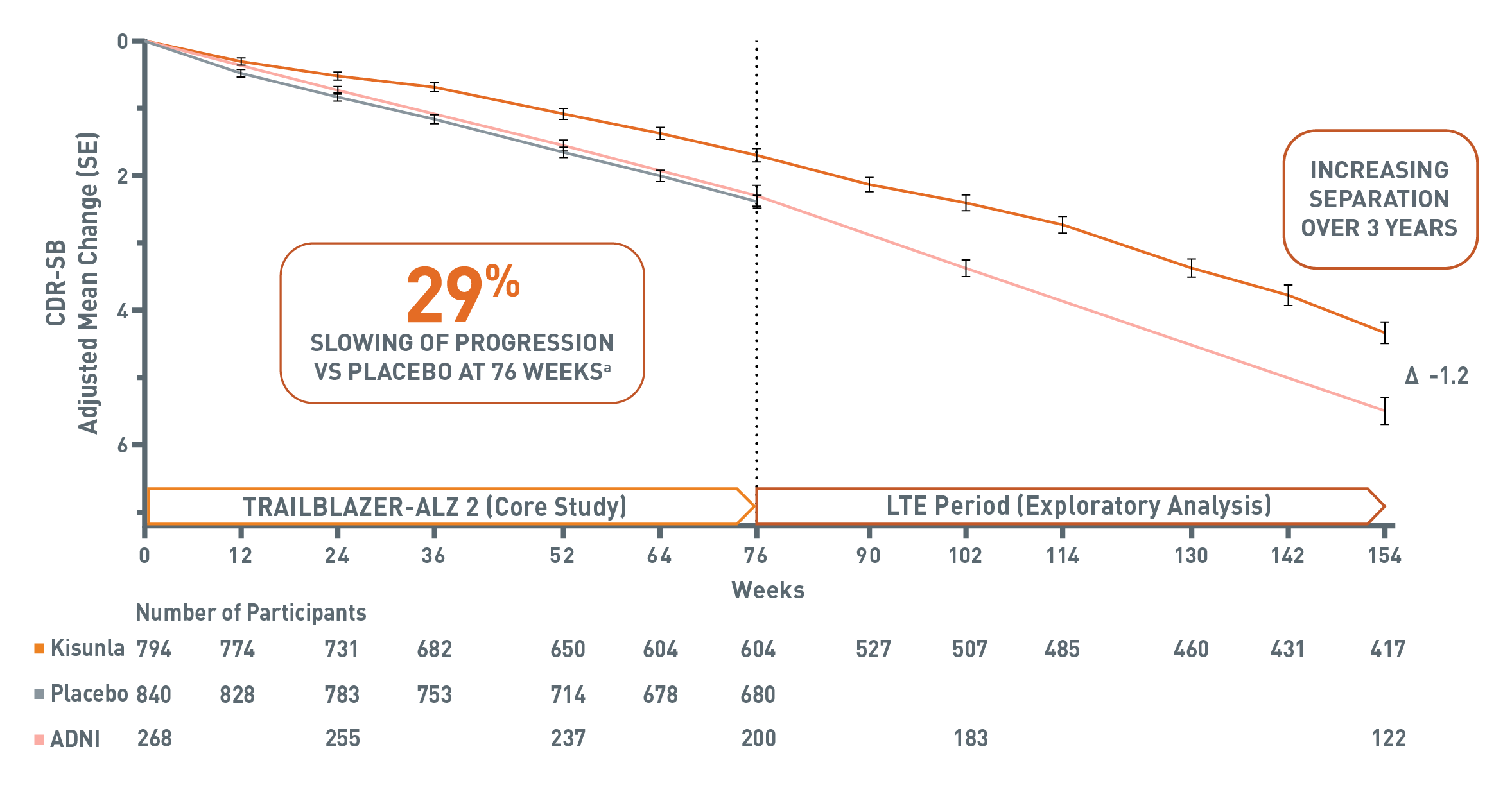
Chart showing the Clinical Dementia Rating Scale-Sum of Boxes (CDR-SB) change from baseline in cognition and function through 154 weeks in the overall population of TRAILBLAZER-ALZ 2 and the Alzheimer's Disease Neuroimaging Initiative (ADNI) cerebrospinal fluid (CSF) group.
At week 0, there were 794 participants in the Kisunla group, 268 patients in the ADNI CSF group, and 840 participants in the placebo group. At Week 52, there were 650 participants in the Kisunla group, 237 participants in the ADNI group, and 714 participants in the placebo group. At Week 76, there were 604 participants in the Kisunla group, 200 participants in the ADNI group and 680 participants in the placebo group. During TRAILBLAZER-ALZ 2 (the 76-week Core Study), participants on Kisunla achieved a 29% slowing of progression vs placebo on CDR-SB. In the overall population, as assessed by mixed model for repeated measures (MMRM) analysis (Kisunla: n=860 and placebo: n=876), Kisunla slowed decline by 29% (-0.70) vs placebo on CDR-SB (P<0.0001 vs placebo). Mean baseline: 3.92 for Kisunla and 3.89 for placebo; change from baseline: 1.72 for Kisunla and 2.42 for placebo.
The long-term extension (LTE) period (exploratory analysis) began at week 76 and ended at week 154. At week 102, there were 507 participants in the Kisunla group and 183 participants in the ADNI group. At week 154, there were 417 patients in the Kisunla group and 122 participants in the ADNI group. At week 154, the difference between the Kisunla group and the ADNI (CSF) group is -1.2.
aIn the 76-week TRAILBLAZER-ALZ 2 Core Study, in the overall population, as assessed by MMRM analysis (Kisunla: n=860 and placebo: n=876), Kisunla slowed decline by 29% (-0.70) vs placebo on CDR-SB (P<0.0001 vs placebo). Mean baseline: 3.92 for Kisunla and 3.89 for placebo; change from baseline: 1.72 for Kisunla and 2.42 for placebo.1
The LTE has limitations, including no placebo control and patients remaining in the extension phase may be those with better results in the Core Study. This retrospective analysis was not a head-to-head study and conclusions cannot be drawn due to potential selection bias, small sample size, and lack of statistical powering.10
Alzheimer's Disease Neuroimaging Initiative (ADNI) is a US and Canadian research study that follows the natural progression of Alzheimer's disease. An ADNI cohort (N=268 at baseline, followed for 36 months) was selected to match participants from the Core Study population based on baseline demographic, clinical, and biomarker characteristics, as detected by cerebrospinal fluid, for use as a reference cohort in the TRAILBLAZER-ALZ 2 long-term extension study. ADNI participants were not enrolled in the TRAILBLAZER-ALZ 2 Core Study or its long-term extension; they were used exclusively as a historical control group.10
CDR-SB=Clinical Dementia Rating Scale-Sum of Boxes; CSF=cerebrospinal fluid; MMRM=mixed model for repeated measures; PET=positron emission tomography; SE=standard error.
SELECT IMPORTANT SAFETY INFORMATION
Hypersensitivity: Kisunla is contraindicated in patients with known serious hypersensitivity to donanemab-azbt or to any of the excipients. Reactions have included anaphylaxis.
KISUNLA DEMONSTRATED REDUCTION IN AMYLOID PLAQUES AS EARLY AS 6 MONTHS1,13*
Amyloid Plaque Reduction From Baseline in the Overall Population in TRAILBLAZER-ALZ 21,13

Nearly half of patients were able to complete treatment course by 1 year based on removal of amyloid plaques to minimal levels on amyloid PET imaging.1,12 Patients treated with placebo had an average of <1% amyloid plaque reduction from baseline to 18 months.13
In patients treated with Kisunla: 17% (130/761) achieved stopping criteria at 6 months, 47% (313/672) at 12 months, and 69% (429/620) at 18 months. In the protocol, if the amyloid plaque level was <11 Centiloids on a single PET scan or 11 to <25 Centiloids on 2 consecutive PET scans, the patient was eligible to be switched to placebo. Amyloid PET values may increase after treatment with Kisunla is stopped. There is no data beyond the 76-week duration of the clinical trial to guide whether additional dosing with Kisunla may be needed for longer-term clinical benefit.1,12
*Mean baseline (n=712) amyloid plaque level for patients treated with Kisunla was 103.7 Centiloids (placebo was 101.4 Centiloids). The mean change from baseline was -62.8 Centiloids at 6 months (n=702), -82.8 Centiloids at 12 months (n=627), and -86.9 Centiloids at 18 months (n=571).1,11
For reference, <24.1 Centiloids on an amyloid PET scan is consistent with a negative visual read.3
PET=positron emission tomography.
NEARLY HALF OF PATIENTS WERE ABLE TO COMPLETE TREATMENT COURSE* BY 1 YEAR1
Percentage of Patients in the Overall Population That Completed Treatment Course* at 12 and 18 Months1,12†

In patients treated with Kisunla: 47% (313/672) completed treatment course at at 12 months and 69% (429/620) at 18 months.
Kisunla treatment course was completed based on removal of amyloid plaques to minimal levels on amyloid PET imaging in TRAILBLAZER-ALZ 2.1
*In the protocol, if the amyloid plaque level was <11 Centiloids on a single PET scan or 11 to <25 Centiloids on 2 consecutive PET scans, the patient was eligible to be switched to placebo. Amyloid PET values may increase after treatment with Kisunla is stopped. There are no data beyond the 76-week duration of the clinical trial to guide whether additional dosing with Kisunla may be needed for longer-term clinical benefit.1
For reference, <24.1 Centiloids on an amyloid PET scan is consistent with a negative visual read.3
†The mean baseline amyloid levels for patients treated with Kisunla were 103.5 Centiloids for the overall population, and 102.4 Centiloids for the low-medium tau population.2
PET=positron emission tomography.
PATIENTS WHO COMPLETED KISUNLA TREATMENT COURSE BY 1 YEAR IN THE CORE STUDY CONTINUED TO DEMONSTRATE SUSTAINED SEPARATION IN CDR-SB SCORES THROUGH 3 YEARS10
Nearly half of patients were able to complete treatment course* by 1 year in the Core Study1
CDR-SB Change From Baseline Score Among Participants Who Met Completion Criteria by 1 Year10,14
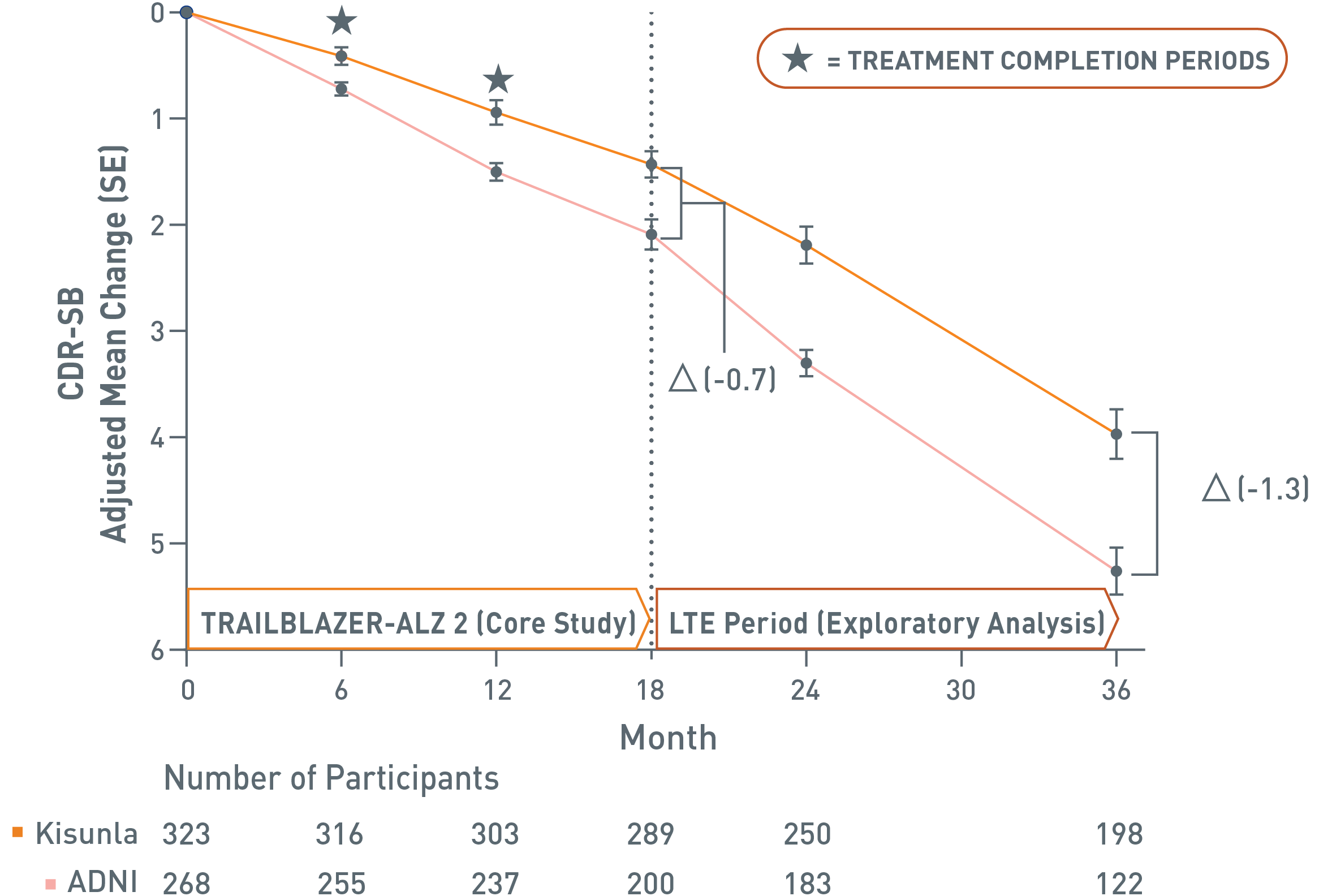
Chart showing the Clinical Dementia Rating scale Sum of Boxes (CDR-SB) change from baseline in cognition and function through 36 months in the donanemab-treated population of TRAILBLAZER-ALZ 2 and the Alzheimer's Disease Neuroimaging Initiative (ADNI) group. Lower values indicate less worsening. At week 0, there were 323 participants in the Kisunla group, and 268 participants in the ADNI group. At 6 months, there were 316 participants in the Kisunla group, and 255 participants in the ADNI group. At 12 months, which is when almost half of Kisunla participants had completed treatment, there were 303 Kisunla participants and 237 ADNI participants remaining in the analysis. At 18 months, the point at which the long-term extension (LTE) period began, there were 289 participants in the Kisunla group and 200 participants in the ADNI group. At 18 months, the Kisunla group showed a slower rate of decline compared to ADNI, the difference in decline between the groups was -0.7.
Stars are included on the chart to indicate when treatment periods were completed. The first is shown at 6 months, the second at 12 months.
The LTE period (exploratory analysis) began at 18 months and ended at 36 months. At 24 months, there were 250 participants in the Kisunla group and 183 participants in the ADNI group. At 36 months, there were 198 participants in the Kisunla group and 122 participants in the ADNI group. At 36 months, the difference in CDR-SB change from baseline was -1.3, demonstrating sustained separation in CDR-SB scores through 3 years.
This exploratory subgroup analysis of the Core Study and long-term extension has limitations, including no placebo control and patients remaining in the extension phase may be those with better results in the Core Study. This retrospective analysis was not a head-to-head study, and conclusions cannot be drawn due to potential selection bias, small sample size, and lack of statistical powering.10
Alzheimer's Disease Neuroimaging Initiative (ADNI) is a US and Canadian research study that follows the natural progression of Alzheimer's disease. An ADNI cohort (N=268 at baseline, followed for 36 months) was selected to match participants from the Core Study population based on baseline demographic, clinical, and biomarker characteristics, as detected by cerebrospinal fluid, for use as a reference cohort in the TRAILBLAZER-ALZ 2 long-term extension study. ADNI participants were not enrolled in the TRAILBLAZER-ALZ 2 Core Study or its long-term extension; they were used exclusively as a historical control group.11
*In clinical trials, completion of active treatment was based on amyloid PET levels measured at week 24, week 52, and week 76. If amyloid plaque level was <11 Centiloids on a single PET scan or 11 to <25 Centiloids on 2 consecutive PET scans, subjects taking Kisunla were eligible to switch to placebo.1,2 The percentages of patients who completed treatment course based on amyloid PET levels at week 24 and week 52 were 17% and 47%.1
For reference, <24.1 Centiloids on an amyloid PET scan is consistent with a negative visual read.3
CDR-SB=Clinical Dementia Rating Scale-Sum of Boxes; PET=positron emission tomography.
SELECT IMPORTANT SAFETY INFORMATION
Amyloid-Related Imaging Abnormalities (ARIA)
ARIA usually occurs early in treatment and is usually asymptomatic, although serious and life-threatening events, including seizure and status epilepticus, can occur. ARIA can be fatal. When present, reported symptoms associated with ARIA may include, but are not limited to, headache, confusion, visual changes, dizziness, nausea, and gait difficulty. Focal neurologic deficits may also occur. Symptoms associated with ARIA usually resolve over time.
References:
- Kisunla (donanemab-azbt). Prescribing Information. Lilly USA, LLC.
- Sims JR, Zimmer JA, Evans CD, et al; for TRAILBLAZER-ALZ 2 Investigators. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527.
- Navitsky M, Joshi AD, Kennedy I, et al. Standardization of amyloid quantitation with florbetapir standardized uptake value ratios to the Centiloid scale. Alzheimers Dement. 2018;14(12):1565-1571.
- Data on File. Lilly USA, LLC. DOF-DN-US-0053.
- Zimmer J, Biffi A, Collins EC, et al. Insights from TRAILBLAZER-ALZ 2 (donanemab): potential clinical translation. Presented at: Alzheimer’s Association International Conference (AAIC); July 28-August 1, 2024; Philadelphia, PA.
- Data on File. Lilly USA, LLC. DOF-DN-US-0064.
- Data on File. Lilly USA, LLC. DOF-DN-US-0074.
- Data on File. Lilly USA, LLC. DOF-DN-US-0073.
- Data on File. Lilly USA, LLC. DOF-DN-US-0076.
- Zimmer JA, et al. J Prev Alzheimers Dis. Published online December 1, 2025(Incl suppl mat).
- Eli Lilly and Company. TRAILBLAZER-ALZ 2 long-term extension preliminary results. Presented at: AAIC; March 2025.
- Data on File. Lilly USA, LLC. DOF-DN-US-0049.
- Data on File. Lilly USA, LLC. DOF-DN-US-0029.
- Data on File. Lilly USA, LLC. DOF-DN-US-0091.